Spinal Cord Stimulation (SCS) in Complex Pain: What You Need to Know

Let’s Talk About Spinal Cord Stimulation (SCS)
Spinal Cord Stimulation is not new, but it is increasingly relevant in the compensation space. As someone who sees complex pain presentations every day, I can tell you that Spinal Cord Stimulation often emerges at a crossroads: where pain has become entrenched, rehab is faltering, and conventional treatments have run their course.
For third-party payers, legal professionals, and rehab teams, this is often the point where questions arise: Is SCS appropriate? Who decides? What’s the evidence?
This short guide is designed to answer those questions, and to show how independent pain assessments can help you navigate high-stakes treatment decisions with more clarity.
What Exactly is SCS—and When Do We Use It?
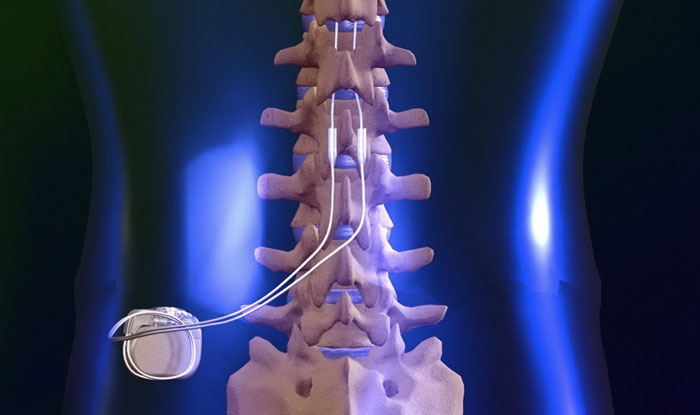
Spinal Cord Stimulation works by sending low-level electrical impulses to the spinal cord to disrupt pain signals. It is most commonly considered for:
- Failed Back Surgery Syndrome (FBSS)
- Complex Regional Pain Syndrome (CRPS)
- Persistent radicular or peripheral neuropathic pain
What is important to understand is that it is not a first-line treatment. It is reserved for carefully selected individuals, usually those who have already tried medications, injections, physiotherapy, psychology and who still have debilitating neuropathic pain that is disrupting their life.
A short trial (typically 5–7 days) precedes permanent implantation. No benefit? We stop there. Good response? We consider the next step.
Who’s a Candidate? What I Usually Look For
In my assessments, I look for a clear clinical picture. It usually includes:
- Neuropathic (“nerve “) pain for more than 3–6 months
- Documented failure of reasonable conservative therapies
- Functional impairment that’s stopping someone from working, caring for themselves, or participating in life
- Psychological readiness—no major unmanaged psychiatric conditions, and insight into the process
- Realistic goals and motivation
In short, I look for a person with persistent pain, realistic expectations, and something meaningful to gain in terms of function.
When SCS Isn’t the Right Fit – What We Look to Avoid:
Equally important is identifying when SCS may not be clinically appropriate or simply not a good use of resources. Often the timing or context is not right. In these cases, it is just as valuable to give stakeholders a clear, well-reasoned “no”.
Common red flags include:
- Predominantly mechanical or nociceptive pain (e.g. axial low back pain without neuropathic features)
- Poorly defined pain diagnoses, overlapping syndromes, or mixed pain states
- Unmanaged psychological conditions, especially severe mood disorders, trauma, or substance misuse
- Passive coping styles or lack of treatment engagement
- Unrealistic expectations, e.g. “I want my pain gone” or “I need this to go back to heavy work tomorrow”
- Early in the treatment journey, where more conservative, evidence-based therapies have not been fully trialled
- In these cases, I will focus on clarifying the diagnosis, recommending alternative strategies (like multidisciplinary rehab, medication optimisation, or pain psychology), and preventing unnecessary escalation.
- Sometimes, saving a patient from an invasive procedure they are not ready for is the most valuable thing we can do.
Why Stakeholders Should Care and What the Data Says
- The clinical results are compelling when the right patient is chosen.
- Well-designed studies show that with careful selection >50% pain relief can be achieved in nearly 80% of FBSS patients, with sustained benefits over 12 months (1)
- Others show the potential for reducing healthcare utilisation and cost “break – even” at 18- 24, especially when it replaces ongoing opioid use or repeated interventions (2)
- In practice, we often see improvements not just in pain scores, but in sleep, mobility, mood and the ability to return to meaningful roles.
How SCS Fits into the Compensation Landscape
Depending on your role, here is how SCS assessments may support your work:
➤ Case Managers
An objective assessment can help clarify treatment direction when rehab is stalling or plateauing. A well-timed assessment can also prevent delay, avoid unnecessary treatment, and redirect care to where it’s most effective.
➤ Legal Professionals (Plaintiff & Defence)
For both sides, independent evaluation helps strengthen your argument, whether supporting funding, contesting necessity, or defining prognosis and cost burden.
➤ Insurers
You are managing risk, and SCS is a big-ticket item. The role of independent assessor is to give you a grounded, evidence-informed opinion: Is it medically appropriate? Is the patient ready? What’s the likely outcome?
Neurostimulation is extensively used for pain control, but it is also used in non-painful medical conditions like pacemakers, which restore abnormal heart rhythms, and cochlear implants, which restore hearing. Spinal cord stimulation was first used to control pain in 1967.
The technology has improved vastly over the years, to the point that they can now even be inserted with minimal discomfort.
Neurostimulation could be considered the game-changer in pain medicine because it has the ability to significantly reduce and sometimes eliminate chronic pain in some people. It does this by ‘closing the gate’ to pain signals that travel up the spinal cord. Neurostimulation when used for pain control, blocks the pain signals as they travel up the spinal cord.
Forms of Spinal Cord Stimulation
Spinal cord stimulation that is used for pain relief includes:
- Spinal cord stimulation (SCS)
- Sacral nerve stimulation (SNS)
- Dorsal root ganglion (DRG) stimulation
- Occipital nerve stimulation (ONS)
- Peripheral nerve stimulation (PNS)
- Peripheral nerve field stimulation (PnFS)
Spinal cord stimulation treatment is generally reserved for severe hard to manage neuropathic pain. Conditions typically treated by this pain treatment include:
- Postoperative persistent syndrome (POPS) (also called failed back surgery syndrome (FBSS), post laminectomy or spinal fusion pain)
- Complex regional pain syndrome (CRPS) (previously called reflex sympathetic dystrophy (RSD)
- Abdominal or visceral pain like angina (some cases only)
- Chronic peripheral ischaemic pain
- Pelvic pain
- Peripheral nerve damage
- Peripheral neuropathic pain
- Phantom limb pain
- Refractory angina pectoris
A Case Snapshot
Meet “Daniel” (name changed), a 45-year-old former scaffolder.
Daniel had two spinal surgeries over three years. He developed chronic lumbar radiculopathy, burning leg pain, sleep disruption, and could not walk his dog around the block. He was on long-term opioids, disengaged from rehab, and stuck in a compensation dispute.
By the time of assessment, it was clear he had exhausted conservative options. But he was also thoughtful, motivated, and desperate for function, not just pain relief.
He trialled SCS and reported a 70% improvement in pain and sleep. His mood lifted. Within months of permanent implantation, he was off opioids, doing home maintenance again, and walking daily. He did not return to scaffolding, but he did return to light part-time work and, more importantly, reclaimed agency over his life.
This is the kind of outcome we aim for. However, it only works if we identify the right person, at the right time, for the right reasons.
Author:
Dr Slava Poel | Pain Medicine Specialist
Independent Medicolegal Assessor
Telehealth Australia-wide assessments
In-person consults Victoria (Vic-WorkSafe, AMA4 (PIEF)
Queensland, ACIME (AMA5)


