Back injury and the urinary system – Dr Jian Cheng
This article discusses the role of back injury in the urinary system by expert Nephrologist, Dr Cheng.

Key points in this article discussed include how:
- Back injury may cause incontinence because continence is maintained by brain, spinal cord, nerves and bladder
- The underlying cause of incontinence is important in referring to the appropriate permanent assessor
- Anti-inflammatory use can cause short and long term damage to kidney function
- Drug accumulation causing side effects may occur in those with kidney impairment
Anatomy and physiology of the urinary system
The urinary system has two phases: storage and voiding. The storage phase allows the bladder filling with urine. During this time, outflow sphincters are closed. This keeps urine from leaking. When the bladder becomes full, stretch receptors in the bladder alert several areas within the brain. At an appropriate time the brain’s control centre coordinates the voiding phase. This involved relaxation of sphincters and contraction of the bladder muscle causing urine to be expelled.
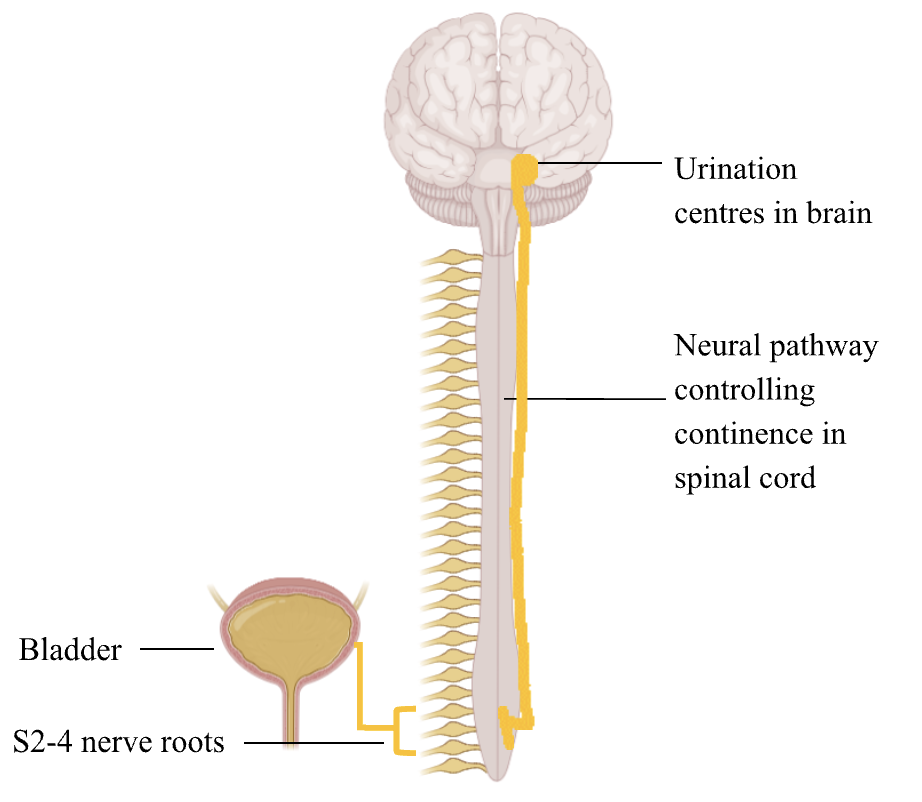
This everyday action is an interplay between the brain, spinal cord, motor and sensory nerves (mostly from the lower nerve roots) and bladder (Figure 1). Therefore, injury to any of these pathways can cause incontinence. The spinal nerves as low as the sacrum level (S2-4) are involved in continence. A common memory aid used in medical school to remember this is “S2-4 keeps waste products off the floor”. Therefore, any disruption between the brain and this level (ie most of the spinal cord) may cause incontinence.
You may read some red flags in assessing back pain in medical reports. These include:
- Incontinence – This implies significant disruption of the neural pathway connecting the bladder to brain
- Saddle anaesthesia – This refers to the area between the legs (which would be in contact riding a horse saddle) becoming numb. The saddle area is also innervated by the sacrum level spinal cord. Therefore damage here may be associated with incontinence
- History of cancer – This question is asked as the doctor is thinking about the possibility of progressive cancer causing back pain or compressing the surrounding nerves
- History of IV drug use – This question is asked as the doctor is thinking about the potential of an abscess causing back pain or compressing the surrounding nerves
Assessing Whole Person Impairment (WPI) Regarding Urinary Incontinence
It is important to medicolegal team to understand the underlying cause of urinary incontinence because it affects accurate calculation of WPI. There are multiple chapters assigning different WPIs for incontinence in the Guides to the Evaluation of Permanent Impairment. The most appropriate assessor depends on the underlying cause. Those whose incontinence is caused by bladder injury should be reviewed by a permanent assessor in the “urinary and reproductive system”. Those whose incontinence is caused by a brain injury should be reviewed by a permanent assessor accredited in “nervous system”. Those whose incontinence is caused by back injury should be reviewed by a permanent assessor accredited in “spine”.
Concrete examples include:
- Case 1: A claimant who had bladder trauma after a machinery accident. This has caused stress incontinence. This claimant should be reviewed by a permanent assessor in the “urinary and reproductive system” with the relevant AMA chapter, as direct trauma to the bladder is the underlying cause for incontinence. Claimants may be assessed up to 70% of WPI.
- Case 2: A claimant who suffered a stroke. They have ongoing urinary incontinence requiring the use of incontinence pads, as well as arm and leg weakness. This claimant is best reviewed by a permanent assessor with “nervous system” accreditation with the relevant AMA chapter. This is because the underlying cause of incontinence is the brain. Claimants may be assessed up to 60% of WPI.
- Case 3: A claimant who had tetraplegia after a car accident, resulting in vertebral fractures causing spinal cord injury. This has resulted in total bowel and bladder incontinence. This patient should be reviewed by an assessor with “spine” accreditation with the relevant AMA chapter. This is because the cause of the incontinence is related to the spinal cord injury – claimants may be assessed up to 60% WPI.
The three cases above demonstrate that even though the claimants all have incontinence, the relevant assessor should be based on the underlying cause. This is important because correct assignment to permanent assessor results in the most accurate WPI calculation.
Pain medications and the kidney
The kidneys have a bidirectional relationship with pain medications, and therefore have relevance in the medicolegal arena.
Pain medications used in back injury can cause short or long term decrease in kidney function. Standard treatment in back injury usually includes anti-inflammatories. There are a wide variety of drugs: common examples in our supermarkets include ibuprofen (brand names Nurofen, Advil), and diclofenac (brand name Voltaren). As a side effect, these drugs can decrease the pressure into the kidney. By doing so, the kidney function may drop. This is amplified in those taking medications with this same side effect. This includes specific blood pressure medications (Common brand names may include Coversyl, Olmetec, Micardis, Tritace) and water pills (such as frusemide, hydrochlorothiazide).
The combination of anti-inflammatory, blood pressure medication and water pill is known as the “triple whammy”. The drop in kidney pressure is compounded, causing kidney injury. Further, long term use of anti-inflammatories can cause chronic kidney disease. These scenarios may be cause for medicolegal action. If permanent injury eventuates, there is also scope for this to be quantified as WPI.
Further, pain medications used in back injury may also accumulate in those with kidney disease. This is because the kidneys are a key component in removing drugs from the body. Some patients with back injury experience nerve pain (characterised by shooting, electric shock-like pain). They may be on medications such as pregabalin (brand name Lyrica) or gabapentin (Neurontin). These medications need to be used carefully in those with kidney impairment. This is because the kidneys are significantly involved in excretion. Therefore, kidney impairment leads to slower clearance. This can cause the toxic accumulation of these drugs. Symptoms of toxicity include confusion, drowsiness and seizures. Prescription below the standard of care may result in medico-legal involvement.
Summary
Urinary continence is preserved by a complex system involving the brain, spinal cord, nerves and bladder. Back injury may cause disruption to this system, resulting in incontinence. The appropriate permanent assessor is dependent on the underlying cause of incontinence. There is a bidirectional relationship between pain medications and the kidneys. Pain medications may cause kidney damage. Kidney damage may potentiate drug toxicity. These may potentiate medicolegal action.
About the Author:
Dr Jian Cheng
Dr Jian Cheng is a dual expert Nephrologist and General Medicine Physician with SIRA Impairment Assessor in kidneys/urology.
Dr Cheng has a keen commitment to holistic patient-centred care, with an emphasis on empowering individuals living with kidney disease.
Australian Specialist Hub is Australia’s leading provider of expert opinion and consulting services to the legal, government, public and private sectors. Serving plaintiff and defendant litigators, in-house legal counsel, insurers, claims managers, loss adjusters and public sector agencies, we provide suitably qualified experts with the required professional, technical, and clinical experience to provide evidence-based reports. Contact our team for more information.


